Hospital discharge is one of the most vulnerable moments in a patient’s recovery journey. Hospital discharge directives guide this transition, but many families in St. Augustine and Palatka don’t fully understand what they mean or how to use them.
At Family, Estate & Mediation Law, we’ve seen firsthand how poor discharge planning leads to preventable complications and readmissions. This guide walks you through what discharge directives are, how to prepare for them, and how to avoid common pitfalls that send patients back to the hospital.
Understanding Hospital Discharge Directives
What Discharge Directives Actually Mean
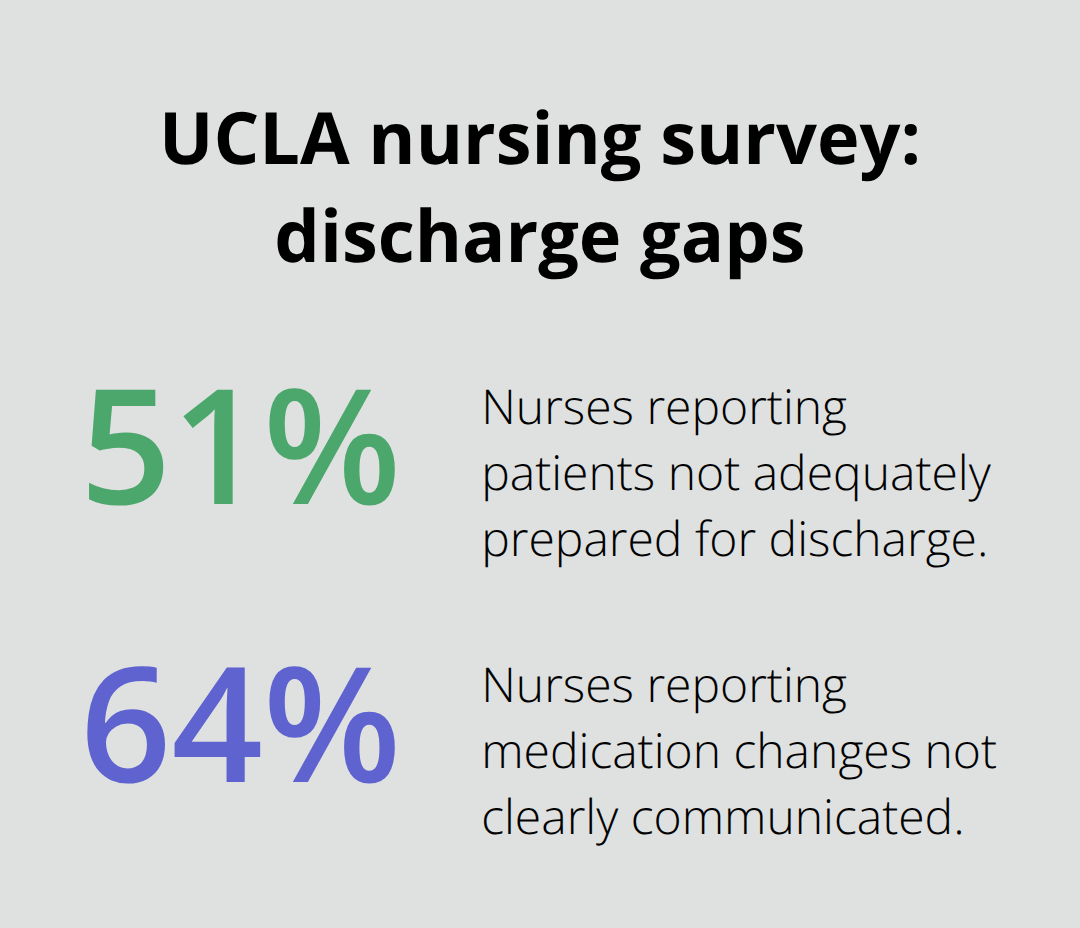
Discharge directives are written instructions that tell you exactly what to do after leaving the hospital. They cover medications, activity limits, diet changes, and when to contact your doctor. The Joint Commission, which accredits hospitals nationwide, requires these directives to be clear and specific. Your physician writes them when you’re medically ready to leave, and they become your roadmap for the next few weeks of recovery. Without them, patients often guess about what they can do, when they can resume normal activities, or which symptoms warrant immediate attention. This guessing game leads directly to preventable readmissions. A UCLA nursing survey of 108 nurses found that 51% reported patients were not adequately prepared for discharge, and 64% said medication changes were not clearly communicated. These gaps happen because discharge planning often starts too late or involves too many different people saying different things.
Why Hospitals Miss the Mark on Timing
Most hospitals hand you discharge paperwork on the day you leave, which is far too late. Research from the Agency for Healthcare Research and Quality shows that starting discharge planning 1 to 2 days before you go home reduces 30-day readmissions significantly. Early planning gives you time to ask questions, arrange transportation, and mentally prepare. The BOOST program, used across multiple hospital systems, cuts readmission rates by about 3% within 12 months by using a simple risk-assessment tool that predicts 90% of readmissions with just two risk factors. This means hospitals can identify high-risk patients early and provide them with extra support before discharge. Families we’ve worked with returned to the hospital within weeks because they didn’t understand their medication schedule or thought chest pain was normal. These situations are preventable.
Medication Management: The Leading Cause of Post-Discharge Problems
Medication errors are the leading cause of post-discharge problems. Most post-discharge adverse events involve medications, according to research published in JAMA Internal Medicine. Your hospital uses medications during your stay, but when you go home, you may need different drugs, different doses, or a different schedule. If your discharge paperwork doesn’t clearly list every medication with its dosage and timing, you’ll make mistakes. A pharmacist should review all your medications before you leave and explain any changes. The CTI (Care Transitions Intervention) program requires a pharmacist-supported medication reconciliation as part of its standard discharge process, and hospitals using this approach have documented cost savings and fewer readmissions. If your hospital doesn’t offer this, ask for it. Write down every medication you take at home, bring that list to the hospital, and ask the pharmacist to compare it with what you’re taking there. Then ask them to write down what you should take when you get home, including any medications to stop or restart.
What Happens When Discharge Planning Fails
Poor discharge planning creates a cascade of problems that extend far beyond the hospital walls. Communication gaps between your hospital team and your home health providers (if you have them) leave critical information lost in transition. Your primary care doctor may not know about medication changes your hospital made, and your home health nurse may not understand your activity restrictions. A UCLA nursing survey found that 60% of nurses agreed there is a lack of effective communication between inpatient and outpatient providers. These disconnects force you and your family to fill in the gaps, often incorrectly. The next chapter covers how to coordinate care between hospital and home to prevent these dangerous communication failures.
Preparing for a Safe Hospital Discharge
Start Coordinating Care Before You Leave
Coordinate your discharge the moment you arrive at the hospital, not the day you leave. Your hospital’s case manager or social worker should meet with you within 24 hours to assess what support you’ll need at home. If no one approaches you, ask your nurse to connect you with case management. This person coordinates everything between the hospital and your home environment, including home health services if you need them. In Northeast Florida, Brooks Rehabilitation Home Health in Palatka offers skilled nursing, physical therapy, occupational therapy, and speech therapy in your home after discharge.
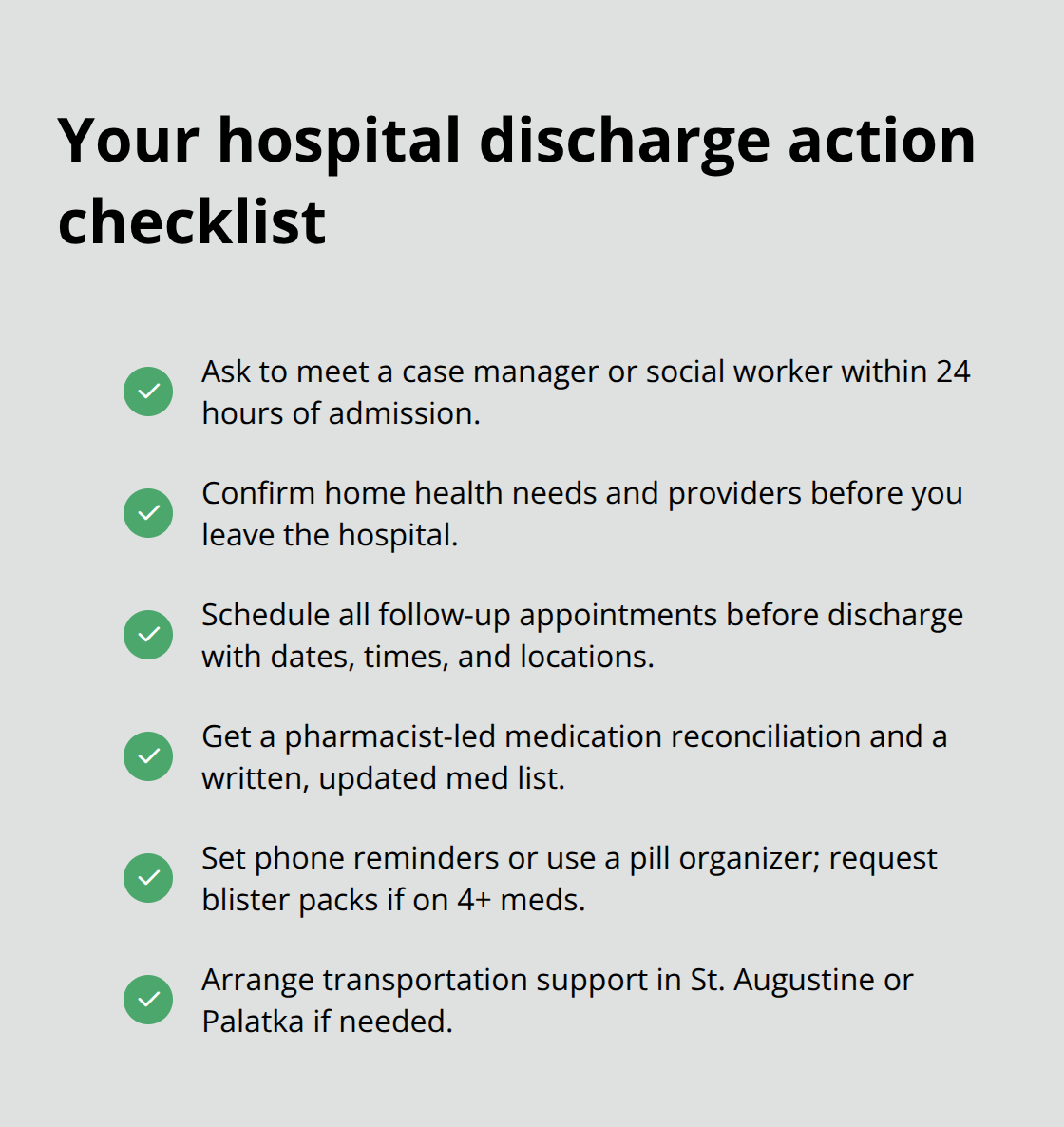
Call (386) 325-4567 to arrange services. Identify what you’ll need before you leave the hospital, not after you’re home struggling to find help.
Research from the Care Transitions Intervention program shows that a 72-hour follow-up visit from a nurse or transitions coach significantly reduces readmissions. This visit happens in your home, where the nurse can see your actual living situation, check your medications, and address questions that arise once you’re managing care yourself. Many families report that everything seemed fine at discharge, then panic set in three days later when symptoms appeared or they realized they didn’t understand their instructions. That panic leads directly back to the emergency room.
Get Your Medications Right Before Leaving
Medications are the single most important thing to get right before leaving the hospital. Ask the pharmacist to sit down with you and compare what you took before hospitalization with what you’re taking now. Write down the name, dose, and time for each medication on a piece of paper you keep in your wallet or purse. Ask specifically which medications from your home supply you should stop taking, which ones to restart, and which are new. This reconciliation prevents the medication errors that cause most post-discharge problems.
When you get home, fill all prescriptions before you run out, not after. Set phone reminders on your phone for each medication time, or use a pill organizer labeled by day and time. If you’re taking more than four medications, ask your pharmacist about a blister pack, where the pharmacy pre-packages each dose for you. Medication errors are the leading cause of post-discharge problems, and most post-discharge adverse events involve medications.
Schedule and Understand Your Follow-Up Appointments
Your follow-up appointments should be scheduled before you leave the hospital, not left as a vague instruction to call your doctor’s office. Ask your discharge nurse to write down the exact date, time, and location of each appointment, plus the phone number to call if you need to reschedule. If you have multiple specialists, your primary care doctor should coordinate communication between them. Many readmissions happen because patients miss follow-ups or don’t understand why they need them.
The BOOST program, used across hospital systems, identifies high-risk patients early and assigns them extra support to attend these appointments. If you have transportation challenges, ask your case manager about community resources or medical transportation services available in St. Augustine and Palatka. Your hospital’s discharge team should address these barriers before you leave, not expect you to solve them alone. Once you understand your medications and appointments, the next critical step involves recognizing what could go wrong and how to prevent it.
Potential Complications and How to Avoid Them
Recognizing Warning Signs After Discharge
The first 30 days after hospital discharge are when most readmissions happen. Research from the Agency for Healthcare Research and Quality shows that structured discharge programs reduce 30-day readmissions significantly, but only if you know what warning signs to watch for and take them seriously. Chest pain, shortness of breath, confusion, fever above 101 degrees, bleeding, severe swelling, or inability to keep food down warrant immediate emergency care. Many families hesitate to call 911 because they think symptoms might be normal after hospitalization, but this hesitation costs lives.
The UCLA nursing survey found that 51% of patients weren’t adequately prepared for discharge, meaning they often don’t know which symptoms are dangerous and which aren’t. Write down the specific warning signs your doctor mentioned before you leave the hospital. Ask your discharge nurse to be explicit about what requires an ER visit versus what requires a call to your primary care doctor versus what you can manage at home. If your hospital doesn’t provide this clarity, contact Brooks Rehabilitation Home Health in Palatka at (386) 325-4567 or ask your primary care doctor to clarify these boundaries with you.
The Care Transitions Intervention program reduces readmissions through structured follow-up and includes a 72-hour home visit specifically to catch problems early before they escalate into full readmissions. Don’t wait for your scheduled follow-up appointment if warning signs appear.
Communication Gaps Between Healthcare Providers
Communication failures between your hospital team and your home health provider create dangerous gaps where critical information gets lost. The UCLA nursing survey found that 60% of nurses agreed there is a lack of effective communication between inpatient and outpatient providers, and 64% said medication changes weren’t clearly communicated. Your hospital discharge summary should go directly to your primary care doctor and any home health agency involved in your care, not sit in a file somewhere.
Call your primary care doctor’s office two days after discharge to confirm they received your hospital discharge summary and understand your medication changes. If they haven’t received it, ask the hospital to send it immediately. Your home health nurse should have the same information. These communication gaps happen because no single person is accountable for making sure information transfers occur. Ask your hospital if they use evidence-based programs that reduce readmissions by clarifying who is responsible for what.
Common Readmission Triggers and Prevention Strategies
Most readmissions within 30 days happen because of medication errors, missed follow-up appointments, infection, or failure to recognize warning signs early. Medication errors are the leading cause of post-discharge adverse events. You prevent this by keeping a written list of every medication with its dose and timing, comparing it to what you took before hospitalization, and asking your pharmacist to explain any changes.
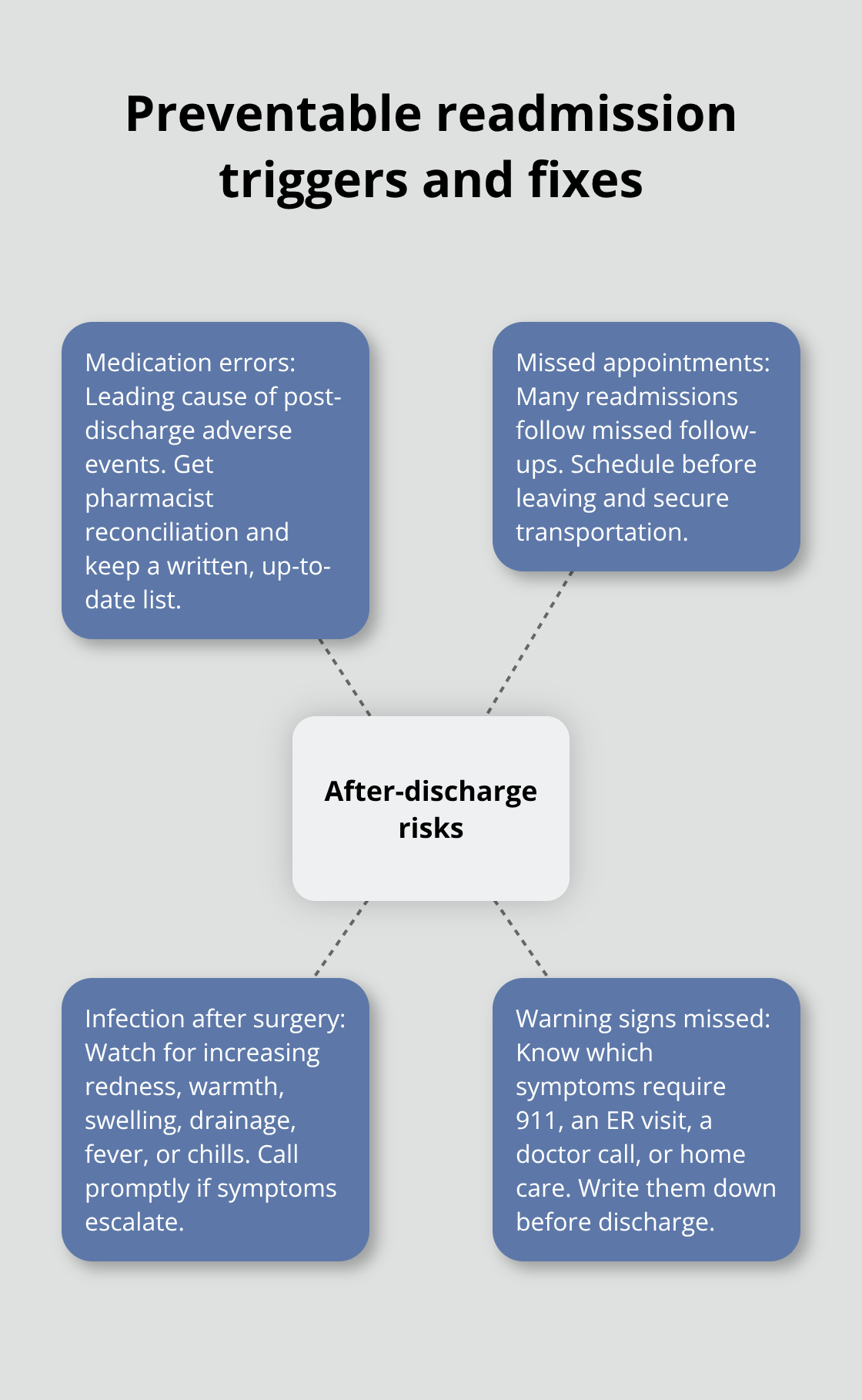
Missed appointments happen because patients don’t understand why they need them or face transportation barriers. Your discharge team should have addressed transportation before you left the hospital. Infection, particularly after surgery, develops gradually, so watch for increasing redness, warmth, swelling, or drainage at surgical sites, plus fever or chills. Failure to recognize warning signs happens because you weren’t told what to watch for. These four triggers account for the vast majority of preventable readmissions, and all four are within your control if you have the right information and support before you leave the hospital.
Final Thoughts
Safe hospital discharge requires action before you leave the hospital, not after. Start discharge planning within 24 hours of admission, obtain medication reconciliation from a pharmacist, schedule follow-up appointments before you go home, and understand which warning signs require immediate attention. Write everything down, compare your pre-hospital medications with what you take now, and confirm your primary care doctor received your discharge summary-these concrete actions prevent the medication errors, missed appointments, and communication gaps that send patients back to the hospital within 30 days.
Northeast Florida offers specific resources to support your transition home. Brooks Rehabilitation Home Health in Palatka provides skilled nursing, physical therapy, and occupational therapy in your home after discharge by calling (386) 325-4567 to arrange services before you leave the hospital. Your hospital’s case manager connects you with community resources in St. Augustine and Palatka, including medical transportation if you need it, and these services bridge the gap between hospital and home when you ask for them during hospitalization.
Hospital discharge directives serve as your roadmap for recovery, but only if you understand them and have the support to follow them. If you face complex family or legal questions related to healthcare decisions, guardianship, or end-of-life planning, Family, Estate & Mediation Law Group can help with practical guidance on estate planning, family matters, and mediation in St. Augustine and Palatka.